Régulation de la pression artérielle
Lorsque le ventricule cardiaque se contracte, le sang est poussé dans les grosses artères ; ici, la présence de tissu élastique et musculaire facilite sa progression et aide à réguler son flux. La pression exercée sur la masse sanguine étire les parois artérielles, qui accumulent de l'énergie élastique pour être libérée lors de la phase diastole suivante (relaxation ventriculaire). L'énergie accumulée pendant la systole est ensuite lentement transférée à la colonne sanguine dirigée vers la périphérie ; ainsi les artères contribuent à transformer les flux sanguins intermittents, venant du cœur, en un flux continu (laminaire), indispensable pour permettre des échanges normaux à niveau capillaire.
Si les parois des artères étaient rigides, la pression systolique s'élèverait rapidement, et laisserait alors place à une « chute tout aussi brutale de la phase diastolique. C'est pourquoi le vieillissement et divers stades pathologiques (comme l'athérosclérose) entraînent une perte de élasticité vasculaire et une augmentation conséquente de la pression artérielle (hypertension).
La régulation régionale du flux sanguin est confiée avant tout aux artérioles qui, grâce à la riche tunique musculaire, peuvent se contracter et diminuer leur lumière jusqu'à ce qu'elle se ferme, ou la relâcher et l'augmenter. Lors d'un exercice physique par exemple, les artérioles de certains quartiers sont obstruées, tandis que celles présentes dans les zones musculaires impliquées dans l'effort physique se dilatent.
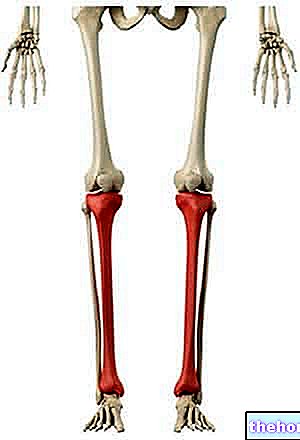
Artères principales du corps humain
D'un diamètre d'environ 2 centimètres et demi, l'artère maximale du corps humain est l'aorte, qui émerge du ventricule gauche du cœur, se présentant comme un tronc ininterrompu qui tend à ne diminuer que vers la fin de son parcours. l'aorte prend des noms différents (aorte ascendante, arc de l'aorte, abdominaux descendants - aorte thoracique) et est à l'origine de nombreux vaisseaux de calibre inférieur dirigés vers différentes régions du corps. À partir de "l'arc de l'aorte", les artères carotide et sous-clavière se ramifient, dirigée respectivement dans la tête et les membres supérieurs ; dans le tractus descendant naît le tronc cœliaque - qui alimente l'estomac, la rate, le foie et le pancréas - les deux artères mésentériques (supérieure et inférieure qui alimentent l'intestin), et les artères rénales dirigée vers les émoncteurs d'organes homonymes. A la hauteur du bassin, la branche descendante de l'aorte subit une ramification, à l'origine des deux artères iliaques communes, qui, après avoir pris naissance les artères iliaques internes dirigées vers le bassin, se prolongent dans les membres inférieurs comme des artères fémorales.
Les artères s'enfoncent généralement profondément dans le corps (sauf dans certaines régions : tempes, poignets, cou), à tel point que de nombreux segments squelettiques reçoivent des empreintes. Les branches formées par les artères sont de deux types : terminales, dues à la bifurcation d'un tronc artériel qui cesse d'exister (par exemple, l'artère brachiale ou humérale, qui se scinde en radiale et ulnaire) et collatérales, qui se détachent d'un "artère qui continue alors son cours. Les vaisseaux artériels sont reliés entre eux par des troncs anastomotiques fréquents, sorte de pontage naturel. Leur présence garantit - dans certaines limites - la vascularisation d'un organe ou d'une partie de celui-ci même lorsqu'une "artère est obstruée. Les anastomoses artérielles sont abondantes dans les organes abdominaux, autour des articulations (où un mouvement peut inhiber l'écoulement dans certains canaux) et dans la zone coronaire.
Les artérioles
La résistance offerte par les artérioles au passage du sang est inversement proportionnelle à leur rayon ; en d'autres termes, plus ils sont dilatés et moins ils offrent de résistance. Mais qu'est-ce qui contrôle la contraction et la relaxation des muscles antérieurs ? Comme prévu, il existe des mécanismes médiés par les nerfs sympathiques (grâce à la libération de noradrénaline), qui régulent la distribution sanguine pour satisfaire certains besoins homéostatiques, tels que la température. Il existe également un contrôle local, dépendant des besoins métaboliques du tissu lui-même, et un contrôle hormonal qui concerne principalement les hormones impliquées dans la régulation de l'excrétion d'eau et de sels par le rein (voir aldostérone, peptide natiurétique auriculaire et vasopressine) Un autre mécanisme intéressant pour réguler le débit sanguin est l'autorégulation myogénique, phénomène par lequel les artérioles soumises à une augmentation de la tension, symptôme d'une élévation de la pression artérielle, se rétrécissent en diminuant le débit qui les traverse.
L'aspect peut-être le plus intéressant qui régule la contraction du muscle lisse vasculaire est le contrôle local susmentionné. Ce mécanisme implique l'endothélium de la tunique intime, qui a la capacité de libérer des médiateurs de la vasoconstriction et de la vasodilatation, mais aussi d'activer les plaquettes. , déclencher un réponse immunitaire et participent aux mécanismes de l'angiogenèse (développement de nouveaux vaisseaux sanguins à partir des vaisseaux existants) et au remodelage des vaisseaux. Parmi ces médiateurs, actuellement l'objet d'une intense étude par les chercheurs, on retiendra le monoxyde d'azote et les radicaux nitrosyle (vasodilatateurs), endothéline et angiotensine II (vasoconstricteurs); le monoxyde d'azote joue également un rôle physiologique important dans le réflexe d'érection du pénis (voir article dédié).
L'activité des artérioles est également régulée par les substances libérées par les cellules locales, ainsi que par les taux plasmatiques d'oxygène et de dioxyde de carbone.En ce qui concerne ces derniers, il est clair qu'une oxygénation réduite traduit la nécessité d'un flux sanguin plus important, à satisfait par la libération du muscle lisse artériolaire. De la même manière, lorsque l'apport tissulaire en oxygène diminue de manière significative, le sang s'enrichit en dioxyde de carbone et en ions H + ; également l'acidose métabolique régionale représente un puissant stimulus à la vasodilatation artériolaire.
Les "métartérioles" commencent immédiatement en aval des artérioles ; ces vaisseaux, pourvus de muscle lisse discontinu, se prolongent à la fois par un certain nombre de capillaires et par des voies vasculaires « collatérales » à visée régulatrice.
Physiologie de la circulation capillaire"