Généralité
La myomectomie est l'opération chirurgicale par laquelle les fibromes utérins sont enlevés.Cette chirurgie est envisagée lorsque les fibromes utérins sont symptomatiques et gênants.
La préparation à la myomectomie est très simple ; de plus, si les instructions du médecin sont strictement suivies, les complications sont rares.

Figure : Types de fibrome utérin
Il existe essentiellement trois techniques chirurgicales que les médecins peuvent utiliser : la laparoscopie, la laparotomie et l'hystéroscopie.
Les résultats sont satisfaisants, même s'il existe un risque de rechute.
Qu'est-ce que la myomectomie ?
La myomectomie est une intervention chirurgicale visant à retirer les fibromes utérins.
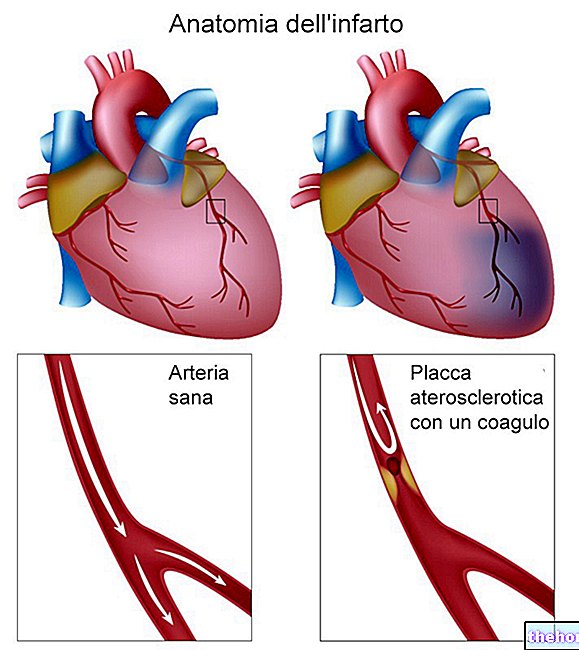
Un fibrome utérin (également connu sous le nom de léiomyome ou myome utérin) est une tumeur bénigne de l'utérus, qui peut se former sur la face interne ou externe de l'organe.
N.B : une tumeur bénigne est une masse anormale de cellules en prolifération qui, contrairement à ce qui se passe dans une tumeur maligne, n'est ni infiltrante ni métastasante (c'est-à-dire qu'elle ne métastase pas).
CARACTÉRISTIQUES PRINCIPALES DES FIBROMES UTÉRINS
Les fibromes utérins sont considérés comme les tumeurs les plus courantes de l'utérus. De forme nodulaire, ils sont constitués d'un petit nombre de cellules musculaires et d'une grande quantité de tissu fibreux.
La taille des fibromes est extrêmement variable : en effet, il existe des fibromes dans l'utérus de quelques millimètres et des fibromes dans l'utérus pouvant atteindre 20 centimètres.
L'apparition d'un ou, plus souvent, d'une série de fibromes utérins altère la structure de l'utérus et diminue sa capacité contractile (la perte de contractilité musculaire est une conséquence naturelle de la présence plus importante de tissu fibreux).
Les fibromes utérins peuvent être asymptomatiques (c'est-à-dire ne provoquer aucun symptôme évident) ou provoquer :
- Règles abondantes et cycle menstruel plus long
- Anémie due à des menstruations plus abondantes (NB : le manque pathologique d'hémoglobine est appelé anémie)
- Douleur et inconfort dans la région pelvienne
- Gonflement abdominal et sensation de lourdeur dans le bas-ventre
- Constipation
- Douleur à la miction
- Douleur pendant les rapports sexuels
- Fertilité réduite et risque accru de fausses couches
Quand tu fais
La myomectomie est réalisée lorsque les fibromes utérins sont symptomatiques (c'est-à-dire qu'ils provoquent un ou plusieurs symptômes) et ne permettent pas à la femme affectée de mener une vie normale. Plus précisément, les situations pour lesquelles l'ablation des fibromes utérins est le plus nécessaire sont :
- Une condition d'anémie persistante et ne répondant à aucun traitement alternatif.
- La présence de douleur ou d'une sensation de lourdeur dans le bas-ventre qui est continue et ne peut être soulagée d'aucune autre manière.
- Une difficulté excessive à tomber enceinte.
La myomectomie est préférable à l'hystérectomie (c'est-à-dire l'ablation complète de l'utérus), car elle préserve l'utérus permettant à la femme opérée en âge de procréer d'avoir des enfants à l'avenir.
Des risques
La myomectomie est sans danger. Cependant, il s'agit toujours d'une intervention chirurgicale, ce n'est donc pas totalement sans risque. Les complications les plus connues sont :
- Saignement excessif (saignement). L'utérus est un organe très vascularisé et l'apparition de fibromes augmente encore le nombre de vaisseaux sanguins présents.Par conséquent, une incision chirurgicale pratiquée sur un utérus dans ces conditions pourrait entraîner une perte de sang importante.
Pour prévenir ou réduire les saignements, les chirurgiens « pincent » souvent les artères utérines momentanément et injectent des médicaments coagulants pour ralentir le flux sanguin jusqu'au point d'opération. - Aggravation de l'état d'anémie. Elle est due à une perte de sang excessive.
- Formation de tissu cicatriciel. Les incisions et coupes chirurgicales envisagées par l'intervention peuvent conduire à la formation d'adhérences intra-abdominales (ou adhérences).Ces dernières sont des bandes de tissu fibreux, qui se créent à la suite du processus de cicatrisation et qui affectent l'anatomie normale de la intérieur des organes.
- Risque accru de complications pendant les grossesses post-opératoires. Après myomectomie, l'utérus devient plus fragile et, en cas de grossesse, peut se rompre au moment du travail. Pour éviter cet inconvénient, le médecin a recours à la césarienne.
- Nécessité d'avoir une hystérectomie.Si la perte de sang de l'utérus est constante et ne peut être arrêtée de quelque façon que ce soit, le médecin peut être obligé d'enlever l'utérus.
QUELLES SONT LES STRATÉGIES UTILES POUR ÉVITER UN SANG GRAVE ?
Pour limiter les pertes sanguines et les effets associés (anémie), en vue d'une future myomectomie, le médecin peut prescrire :
- Un agoniste de l'hormone de libération des gonadotrophines (Gn-RH) ou la pilule contraceptive, pour réguler le cycle menstruel et minimiser la quantité de sang perdue pendant la menstruation.
N.B : un agoniste, en pharmacologie, est un concurrent de la molécule naturelle.
- Une thérapie médicamenteuse capable de réduire le volume des fibromes utérins et de l'utérus.Dans ces conditions, l'organe sur lequel intervenir devient plus petit, tout comme l'incision à faire devient plus petite.
Les médicaments utilisés sont, encore une fois, les agonistes de la Gn-RH ; celles-ci, en effet, produisent une sorte de « ménopause temporaire » : la patiente, en effet, éprouve des bouffées de chaleur, des sueurs nocturnes, une sécheresse vaginale, etc.
Cependant, il faut préciser que cette pharmacothérapie ne concerne pas toutes les femmes : chez certaines, en effet, les fibromes prennent un aspect indiscernable du reste de l'utérus, ils ne sont donc plus reconnus au moment de l'opération.
Préparation
La myomectomie est une intervention chirurgicale qui implique une anesthésie générale ou une rachianesthésie, par conséquent, avant de pouvoir être réalisée, la femme à opérer doit être soumise aux contrôles cliniques suivants :
- Examen physique approfondi
- Prise de sang complète
- Évaluation de l'histoire clinique (maladies subies dans le passé, allergies éventuelles aux anesthésiques, médicaments pris lors des contrôles, etc.)
- Électrocardiogramme
Si aucune contre-indication d'aucune sorte n'apparaît, le médecin explique au patient tout ce qui concerne l'opération, y compris les recommandations pré et post opératoires, le type d'anesthésie envisagée, la technique chirurgicale utilisée, la durée prévue de l'opération et les délais de récupération. .
RECOMMANDATIONS PRÉ-OPÉRATOIRES ET POST-OPÉRATOIRES
Pour que l'ensemble de la procédure se déroule sans heurts, le patient doit :
- Avant la myomectomie, arrêter toute prise médicamenteuse à base d'antiplaquettaires (aspirine), d'anticoagulants (warfarine) et d'anti-inflammatoires (AINS) ; cette interruption est nécessaire car ces médicaments, en diminuant la capacité de coagulation du sang, prédisposent à des hémorragies sévères.
- Le jour de la myomectomie, passez à un jeûne complet au moins la veille au soir, car une anesthésie générale ou une rachianesthésie est nécessaire.
- Après la chirurgie, demandez à un membre de votre famille ou à un ami de vous accompagner à la maison.
Procédure
Selon le nombre, la localisation et les caractéristiques des fibromes utérins, le chirurgien peut réaliser une myomectomie en laparotomie (myomectomie abdominale ou traditionnelle), en laparoscopie (myomectomie laparoscopique) ou en hystéroscopie (myomectomie hystéroscopique).
MYOMECTOMIE ABDOMINALE
La chirurgie réalisée en laparotomie consiste à ouvrir l'abdomen en pratiquant une incision de plusieurs centimètres au niveau du ventre, ce qui rend l'intervention invasive et la phase post-opératoire très longue.

Figure : myomectomie laparoscopique. Depuis le site : en.wikipedia.org
La myomectomie abdominale, qui implique une anesthésie générale, est indiquée pour les utérus recouverts de plusieurs gros fibromes.L'incision sur l'abdomen peut être horizontale ou verticale, selon la localisation et les caractéristiques des fibromes.
Après la procédure, le chirurgien ferme l'abdomen du patient avec des points de suture.
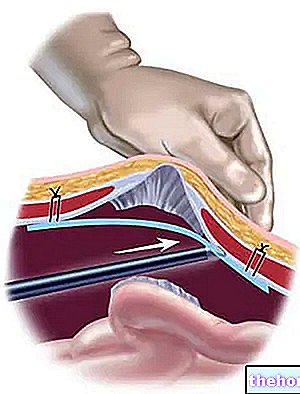
MYOMECTOMIE LAPAROSCOPIQUE
La laparoscopie est une technique chirurgicale mini-invasive, qui permet d'opérer sans pratiquer de grandes incisions cutanées ; l'opération, en fait, comporte deux ou trois petites incisions, qui sont utilisées par le chirurgien pour introduire le laparoscope (un appareil équipé de lumière et de caméra) et les instruments chirurgicaux.
La myomectomie laparoscopique, qui nécessite une anesthésie générale, convient aux utérus comportant jusqu'à deux fibromes, et ceux-ci ne doivent pas mesurer plus de 5 à 6 centimètres et être situés sur la paroi externe de l'utérus (sous-sérose).
Myomectomie robotique
La myomectomie robotisée est une opération laparoscopique dans laquelle le chirurgien, au lieu de s'opérer lui-même, guide un instrument robotique équipé de bras mécaniques, qui, en fait, remplacent ses mains. Cela permet une grande précision de l'intervention.
MYOMECTOMIE HYSTEROSCOPIQUE
La myomectomie hystéroscopique est une technique chirurgicale peu invasive, qui est réalisée en introduisant un instrument spécial appelé résectoscope dans l'utérus par le vagin et le col de l'utérus.
Le résectoscope, en plus d'avoir une lumière et une caméra reliées à un moniteur externe, est équipé d'une source de décharges électriques : ces décharges sont utilisées par le chirurgien pour éliminer le tissu qui constitue les fibromes utérins.
La myomectomie hystéroscopique est indiquée pour les fibromes utérins moyens à gros de type sous-muqueux et peut être réalisée sous anesthésie générale ou rachianesthésie.
EST-IL POSSIBLE D'OPÉRER PENDANT LA GROSSESSE ?
La grossesse peut stimuler l'apparition de fibromes. Ceux-ci sont généralement retirés quelque temps après la naissance, mais il peut arriver, en de rares occasions, qu'ils doivent être retirés peu de temps avant la naissance du bébé.
Phase post-opératoire
La phase post-opératoire dépend du type d'intervention :
- Myomectomie abdominale : comme il s'agit d'une opération très invasive, elle peut nécessiter une hospitalisation de plusieurs jours, voire 3 ou 4. Temps de convalescence attendu : 4 à 6 semaines.
- Myomectomie laparoscopique : nécessitant une anesthésie générale, le patient doit passer au moins une nuit à l'hôpital, pour des raisons de précaution totale.Durée de récupération estimée : 2-3 semaines.
- Myomectomie hystéroscopique : si elle est réalisée sous rachianesthésie, le patient peut sortir quelques heures après l'intervention.Les temps de récupération sont très courts : une semaine, sauf complications.
COMBIEN DE TEMPS APRES L'INTERVENTION PEUT AVOIR UNE GROSSESSE ?
Après une myomectomie, l'utérus met environ 3 mois à guérir complètement : les médecins recommandent donc d'attendre au moins 90 jours avant de tomber enceinte.
Résultats
Les résultats de la myomectomie sont tout à fait satisfaisants.
Très souvent, en effet, les symptômes causés par les fibromes disparaissent et la fertilité augmente. Cependant, il est possible qu'après quelques mois des rechutes apparaissent (c'est-à-dire que les fibromes se reforment) et qu'une deuxième opération de myomectomie soit nécessaire.